















“Houston We Have a Podcast” is the official podcast of the NASA Johnson Space Center, the home of human spaceflight, stationed in Houston, Texas. We bring space right to you! On this podcast, you’ll learn from some of the brightest minds of America’s space agency as they discuss topics in engineering, science, technology and more. You’ll hear firsthand from astronauts what it’s like to launch atop a rocket, live in space and re-enter the Earth’s atmosphere. And you’ll listen in to the more human side of space as our guests tell stories of behind-the-scenes moments never heard before.
Episode 57 features Dr. Zarana Patel, a portfolio lead scientist at NASA’s Johnson Space Center, who is responsible for management and scientific oversight of degenerative tissue risk of space radiation. This is part one of a five-part series on the hazards of human spaceflight. This episode was recorded on June 29th, 2018.
Exploration to the Moon and Mars will expose astronauts to five known hazards of spaceflight, including radiation. To learn more, and find out what NASA’s Human Research Program is doing to protect humans in space, check out the “Hazards of Human Spaceflight” website.

Transcript
Gary Jordan (Host): Houston, We Have a Podcast. Welcome to the official podcast of the NASA Johnson Space Center, Episode 57, Hazard Number One: Radiation. I’m Gary Jordan, and I’ll be your host today. On this podcast we bring in the experts — NASA scientists, engineers, and astronauts — all to let you know the coolest information about what’s going on right here at NASA. So today this podcast, this episode is part one of a five-part series on the hazards of human space flight. So a human mission to Mars is extremely complex and challenging and has hazards such as radiation, isolation and confinement, distance from Earth, gravity, and hostile and closed environments. And they’re being studied in ground-based analogs here on Earth, in laboratories, and of course, on the International Space Station. So today we’re going to talk about that first one, radiation. We’re talking with Zarana Patel, a portfolio lead scientist here at the Johnson Space Center. Zarana is responsible for management and scientific oversight of degenerative tissue risk for the space radiation program element.
So if you missed it, I talked with Dr. Mike Barratt last week. He’s a NASA astronaut. And he gave a nice overview of all five hazards, including radiation. And as a space traveler himself and a medical doctor, he gave a nice two-minute overview of why we’re concerned about radiation in the first place and what we know so far. What exactly — you said, you know, from small effects to, you know, lethal effects of radiation, what exactly is radiation doing to the human body?
This episode is part one of a five-part series on the hazards of human space flight. Today we’re going to talk about that first one, radiation. Zarana Patel, a portfolio lead scientist here at the Johnson Space Center, is responsible for management and scientific oversight of degenerative tissue risk for the space radiation program element.
Mike Barratt:So when we think about space flight radiation, we’re mostly concerned with charged particles, which with electrons and protons and some heavier particles that are basically stellar products coming from supernova explosions and energized gas clouds. And I’ll have to caveat that by saying we also have issues with neutrons because those can be formed by interaction of these heavy particles with structure. But these are traveling very fast and they possess a lot of energy. And so when they hit something that’s of value to us, such as macromolecules like DNA, they can actually induce direct damage. And if you get a large enough dose, they can actually kill cells. It’s some of those smaller doses that we’re a little bit concerned about because they can damage DNA in such a way — in fact, many different ways — that can potentially cause cancers, cause lethality from cancers many years after your exposures. And there’s a lot of uncertainty about what dose of what charged particle will affect — will cause what effect on the human body.
And so that’s one of our major areas of interest in our research.
Host: Do we have radiation studies on the International Space Station?
Mike Barratt:Absolutely. So just like a radiation technologist or a nuclear energy worker, we have a very highly-monitored environment. And every crew member wears a radiation badge, just like any of those people in those industries that I mentioned. We have area detectors which map out the radiation exposure of each area of the Space Station. We have furthering our suite of detectors, charged particle directional detectors, which tell you what the charges are and from what direction they come. And those are the particles that come in from the sun and from galactic cosmic rays. And, of course, we have our ground observations. We composite all those together along with satellite data as well and we get the best picture we can of the radiation environment for low-earth orbit.
Host: So that clip was from last week’s episode. It was called Dr. Spaceman, where we go through Dr. Barratt’s story and an overview of the five hazards. But today we’re diving deep into the first part on radiation with Dr. Zarana Patel. So with no further delay, let’s go right to it. Enjoy.
[ Music ]
All right, Zarana, thank you so much for joining me today to talk about radiation.
Zarana Patel:You’re welcome. Thank you for having me.
Host: You’re welcome. This is an interesting, interesting concept. Because it’s something that I think is one of the main concerns, I would almost assume, whenever people talk about, “Well, what do we need to be worried about whenever we go out into space?” Radiation is just always one of those things that comes up. But I want to start with a question of why is radiation such a concern? What do we have to be worried about?
Zarana Patel:Yeah. And the real — the pretty significant thing there is that — the type of radiation you’re going to encounter in space is different than the types of radiation we encounter here on Earth. In space you’re exposed to this thing called HZE radiation, so that stands for high-Z, which is atomic mass, and high-E, which is energy. So these — these heavy ions, they have a lot of mass, they have a lot of energy. And in that way they are very different from gamma rays or X-rays that we’re going to see on Earth. They’re densely ionizing, which means that as they move along their target volume, they have the ability to cause a lot of damage within this one core track.
Host: Wow.
Zarana Patel:And they also have these little offshoots from the core track called delta rays. So these delta rays can also go off to neighboring cells or volumes and causes additional damage. So for something sensitive like DNA where one hit can be a point of failure, right, one hit can causes a mutation that can propagate into further damage, it can propagate into cancer. When one hit is a point of failure and you have a lot of complex damage that you can’t repair, it becomes a big problem.
Host: And you’re talking about the human body, right?
Zarana Patel:Mm-hmm.
Host: You’re talking about when this heavy — this space form of radiation hits a living organism?
Zarana Patel:Exactly. The other difference is that in space, there’s a type of dose rate that is in space — it’s different. It’s a lot of chronic exposure, ever-present but at low doses; however, as on Earth you get single X-ray or CT scan, you know, it’s a single 15-minute exposure or an hour exposure and then you’re done until the next time.
Host: Hmm. Yeah, so when I go to the dentist and they do the snapshot, it’s really just a quick second there.
Zarana Patel:Exactly.
Host: Yeah. But this long form — and that’s why, you know, when I go to the dentist, they put on this big lead vest, right, and then they shoot me with radiation. And the dental hygienist is going around the corner because they doesn’t want to be a part of it. So, you know, even just that little bit, everyone’s, like, real nervous about.
Zarana Patel:Yeah. And I think it is important to note that on Earth we have radiation protection standards. So likewise, we would have radiation protection standards for any astronauts we send into space.
Host: And the hard thing would be controlling and keeping those standards with such a persistent presence of it. That’s got to be pretty challenging.
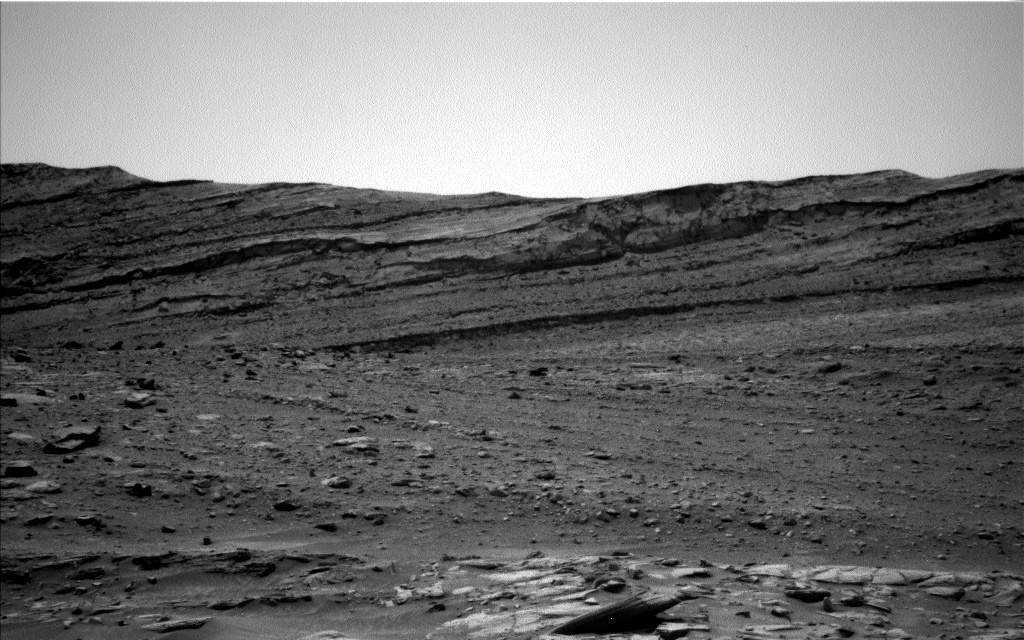
Zarana Patel:The monitoring of it is actually fairly straightforward now. It wasn’t always like that. But now that we’ve developed newer technologies, newer dosimeters, things that measure the radiation, things like the MSL rad tool on Curiosity Rover went from here to Mars. And on its way there, it took radiation — it took measurements of the radiation environment. So now we have a really good idea of what’s happening from here to Mars and on the surface of Mars. So a lot of this data we’re compiling and keeping track of so we understand what the space radiation environment’s going to be like when we actually send humans there and back.
Host: So you understand the environment. I guess where the questions lie is what happens to the human body, right?
Zarana Patel:Yeah, there is huge uncertainty in terms of the biological responses for these space radiation exposures. So that’s where a lot of our research within the Human Research Program focuses on, quantifying the biological responses and then doing what we can to mitigate them.
Host: Right. Yeah, and if I’m going to the dentist and they’re going around the corner when I’m getting blasted with X-rays, I’m sure no one’s really going to sign up to get blasted with radiation to find out what happens to the body.
Zarana Patel:Yeah, no one’s — unfortunately, we cannot irradiate people.
[ Laughter ]
Host: You say that from a scientific perspective.
Zarana Patel:Yes, yes, of course. So we rely heavily on animal and cellular models to gather the evidence we need to characterize a risk from space radiation and to do — evaluate countermeasures.
Host: Okay. So what’s the technique there? What are we doing to find out?
Zarana Patel:Yeah, that’s a great question. Most — most of the elements here at NASA rely on some form of ground analog to do a lot of their testing. And we have a similar one called the NASA Space Radiation Laboratory. It’s housed at Brookhaven National Labs, and it’s basically the top of the line facility, probably the most sophisticated facility in the world where you can simulate space radiation exposures. It also has a nice facility onsite for biological experiments, which is essential since we are using animal and cellular models. So it combines this capability to do long-term animal studies and cellular work along with a heavy ion accelerator.
Host: Hmm. So what do — what do they show us? What are we beginning to understand with these tests?
Zarana Patel:So to date there are four health risks from space radiation exposure that we identified. The first one is cancer. The risk of radiation-induced carcinogenesis, and that includes epithelial cancers and leukemias. And this is actually the biggest contributor to this permissible exposure limit that — that’s the standard we set for our astronauts. The next one is the risk of in-flight and late CNS decrements. So CNS is central nervous system. And basically it’s the risk of behavioral or cognitive decrements either in-flight or late post-mission, which can manifest in neurodegenerative disorders like Alzheimer’s.
Host: Oh, wow.
Zarana Patel:And this one we’re targeting pathology that can have commonalities between those disorders and cardiovascular disease, which brings me to the next risk, which is the risk of radiation-induced cardiovascular disease. But it’s not just cardiovascular disease, it includes things like cataracts and other degenerative tissue effects, such as immune decrements, respiratory and digestive dysfunction, early aging or premature aging. And finally, the last one is the risk of acute radiation syndromes. This is a really specific one for solar fares or what we call solar particle events. So this one is a more intermittent but large dose exposure from a solar flare. And you have things like skin burns, prodromal responses, nausea. This one is fairly effectively shielded against.
Host: Really? Okay. And is it — nausea, it sounds like a short-term thing. It would be like you would go through this blast and it would be sort of a short-term thing. Whereas this sounds like, you know, cancer and cataracts, they seem like very long-term effects.
Zarana Patel:Yeah. There’s these acute effects and there’s these late effects. And the latency between the two can vary, you know, in terms of minutes to decades. So for acute radiation syndrome, you will manifest immediately and over a period of months. But the radiation exposure you get initially will also contribute to your late effects of cancer, [inaudible], and cardiovascular disease. Because your radiation exposures are accumulated.
Host: I see, I see. Now, this is — this has got to be related to a lot of other effects, too. Because, you know, looking at radiation specifically, now there’s all these other hazards that we’re going to talk about in this series, the isolation, distance from Earth, the fluid shifts and some of the effects of the altered gravity that are going to compound based on these radiation. Because radiation — are you looking at other areas as well beyond radiation and how radiation might amplify these effects?
Zarana Patel:Yes, for sure. The chief scientist always likes to say that the body is experiencing this whole body outcome in space; you’re not really experiencing any one of these hazards as a stand-alone. So you have to account for the fact that there might be additive responses, or synergistic responses, or antagonistic responses. So does radiation simply add on with microgravity or altered gravity, or are they synergistic in that they can cause an even larger effect in either two alone or combined? Or do they, when combined, cause a decreased effect? So these are things that we definitely have within our knowledge gaps for these four risks and we do have to evaluate whether or not they’re acting in any kind of interacting manner with these other hazards.
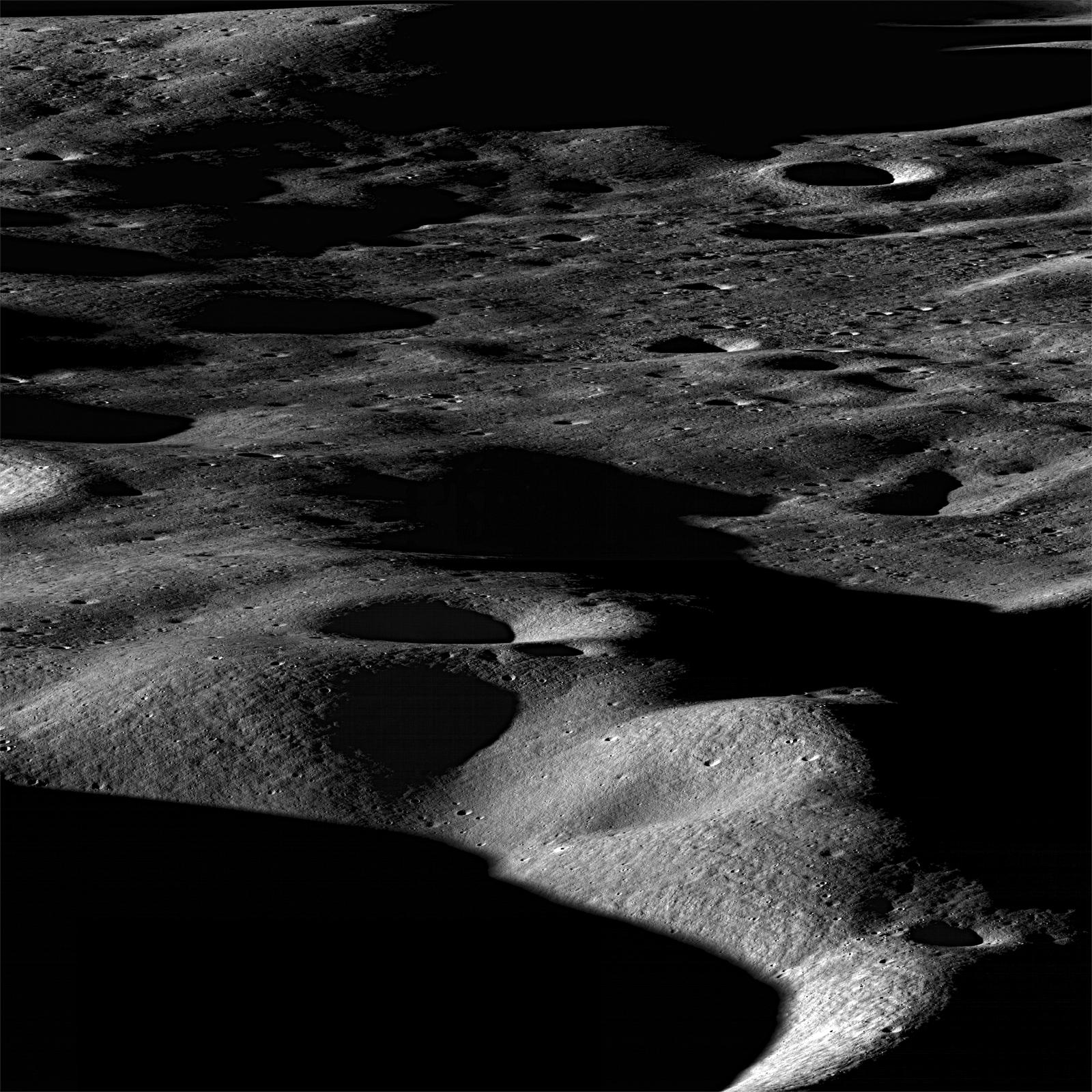
Host: Well, let’s start with kind of what we know starting from the beginning. You know, we’re starting to venture farther into space in the ’60s, especially during the Apollo Program. Apollo 8 was the first time that astronauts actually went past low-earth orbit and now we’re going towards the moon. What is the radiation environment that they sort of went on? And a lot of the other Apollo astronauts after them, too? What was the radiation environment like for them?
Zarana Patel:So with — with the early programs, they were obviously very short durations and they were at relatively lower altitudes. The radiation exposures there were fairly low and their concern was mostly solar particle events. But as the mission architecture changed, you’re going to higher altitudes, longer durations and now beyond low-earth orbit, you do have to account for the galactic cosmic radiation that’s going to be omnipresent. And basically, with increasing time, you have increasing exposure to GCR. So you are going to have a lot of deep space radiation exposures on your way from Earth to Mars and back. You’re going to have to account for that. And then for a three-year Mars mission, it’s going to be about an order of magnitude higher than the current levels of exposures we’re seeing right now on the ISS.
Host: Do we know if the radiation levels would sort of plateau after a certain point and they’ve done their damage and that’s as far as it’s going to go? Or will it be seriously keep being worse and worse the longer that they’re out there?
Zarana Patel:That’s an interesting question. I don’t know if there will be a plateau or not. But I think the question right now of whether or not there’s a threshold dose is important for things like the risk of heart diseases.
Host: Oh, okay.
Zarana Patel:So the heart and cardiovascular system is a fairly — what they call a resistant system. It can take some damage and still output in terms of function normally. So this is called a deterministic risk. There’s a threshold dose at which you will start seeing effects. So current evidence to date suggests that the risk of heart disease has a threshold dose, and right now it might be about half a gray. But as people are reanalyzing the epidemiological data and more data’s coming in, there are suggestions that there actually may be lower and lower thresholds or no threshold at all. That makes it go from a deterministic risk to a probabilistic risk like cancer, which means that any radiation exposure accounts for — includes some level of risk. So, for example, on a Mars mission when you are nearing half a gray levels of radiation exposure, that’s — that’s at the level of a threshold dose of radiation-induced heart diseases. That’s when we become concerned.
Host: Now, what’s a gray? A half a gray, what’s that?
Zarana Patel:So the gray is a standard unit of measure for radiation, how much you’re actually absorbing in your body. But that can be translated in terms of biological effects using some kind of quality factors. So you might absorb half a gray in your body, but biologically your body might feel like it’s one — you might absorb half a gray in your body but biologically your body might feel like you’re getting 1.2 sieverts of damage. And a sievert is sort of this scaling factor or ends up being a scaling parameter to account for quality difference from a space radiation and other Earth exposures. So if you absorb half a gray of radiation exposure, it might feel like one gray of gamma exposure, and that’s what the sievert sort of translates into.
Host: So is — from your perspective, you know, studying radiation and sort of kind of understanding these thresholds, these limits, is there a limit to how long we can spend out in space before we have to come home?
Zarana Patel:Yes, so NASA sets the permissible exposure limits. Right now the limit is at 3% excess read. So it’s 3% excess risk of death from cancer. And this — this excess career limit is the same for both men and women, but the risk function, it’s a function of age at exposure, sex, and smoking status. So we know that the older you are, the less likely you are to have an increased risk of cancer from radiation and exposure. We also know that there’s some evidence suggesting that women are more sensitive to radiation exposure and certain types of cancers as a result than men. So yes, your career limit is going to be the same for all crew, but depending on your age, sex status, and smoking status, the number of safe days that you can spend in space will vary.
Host: Hmm. So I guess Mars missions are going to be pretty tough. That’s several years?
Zarana Patel:Yes, three years is a long time. And the accumulated dose there is going to be pushing the permissible exposure limits that we have right now.
Host: Wow. So what do we know based on some of our studies on the International Space Station? One of the best parts is it’s a platform for understanding how the human body reacts to being in space. Now, there’s a little bit of extra shielding from the magnetic sphere, right, then maybe when we get further out in space. So radiation — I guess we’re still learning a little bit, but I guess not as much as we would in space travel. So what do we know now?
Zarana Patel:In terms of the ISS, the — it’s in low-earth orbit. So like you mentioned, it is protected by the earth’s magnetosphere from a lot of GCR — not all of it, but a lot of it. And the six-month missions and the one-month missions that we’re currently doing, you’re going to receive a fairly low amount of radiation. Of course, if you’re flying multiple missions, they will accumulate, like I mentioned.
Host: Right.
Zarana Patel:So with low-earth orbit, your risk is still within the limits that we set. When you go to the moon and depending on the mission architecture for the moon and then the deep space — deep space sorties, you will be pushing the limits that we set for both men and women. As far as these studies on the ISS, like I said, because these doses are so low, within the human cohort — the human astronaut cohort — you really can’t distinguish a single signal from radiation versus the noise that you’re going to get. So, for example, if you take a look at radiation-induced heart disease, the entire astronaut cohort is probably 350 give or take. If you look at — if you try to identify is there an increased risk of space radiation-induced heart disease in that cohort, you won’t be able to find a signal that is statistically significant. So we know there’s a risk because in epidemiological studies these are human ground studies from terrestrial exposures.
These cohorts sizes go from tens of thousands of people. So when you consider a cohort, that’s 350 to tens of thousand of people, you can better distinguish the signal from the radiation-induced heart disease compared to the noise. So we know that there is a risk, we just can’t identify it in a smaller cohort like the astronaut cohort. So we have to rely heavily on the terrestrial data as well as all the data that we’re going to compile at the NASA Space Radiation Laboratory.
Host: Right. Are you doing different sorts of tests in the NASA Space Radiation Laboratory, or are just doing the same tests with a lot of samples?
Zarana Patel:Yeah, we rely on animal studies mostly. And we have the development of this GCR simulator facility, which will have the capability to cycle through multiple ions and simulate the reference field which is basically what you would experience in space. The GCR reference field in space is very complex. You can have a number of ions represented in that field, you know, maybe up to 20 ions. But on the ground we’re not going to use 20 ions. Maybe we’ll simplify it to five and cycle through them repeatedly to expose animals to that kind of field. You also have to account for the dose rate. You have to give the animals the small dose over a large period of time to simulate the Mars exposure. So those are the kind of tests we’re going to be doing.
Host: So how well do these tests — you know, we’re talking about cells, we’re talking about animals — how well do they translate to what’s going to happen to the human body?
Zarana Patel:Yeah, that is a very good question and one of the biggest challenges that people who use and rely on animal models have in general: How well do these animal and cell data that we’re going to collect translate and how can we translate them to the human condition, to the astronaut condition? So we have to rely on this vertical and horizontal transition paradigm. So vertical translation just means going from bench to bedside. Going from the lab bench, including biologists, chemists, and including all the way up to the top, the clinicians that are going to be implementing this kind of work and interacting with the humans. And then the horizontal translation just means going from different — just being interdisciplinary, multidisciplinary. We’re going to talk to physicists, we’re going to talk to modelers, we’re going to talk to epidemiologists, we’re going to talk to biologists and chemists. We’re going to talk to managers and vehicle design people as well. So you have to include basically this whole entire field to account translation from a cell or an animal to a human.
Host: Right. Because you don’t want to be isolated to just your perspective.
Zarana Patel:No.
Host: This grander perspective really helps you understand what’s going to happen, right?
Zarana Patel:Exactly.
Host: Yeah. So you said you’re mostly from the biological perspective, but, you know, having someone that understands physics maybe a little bit more can help you understand?
Zarana Patel:Exactly. And I think that’s where my bioengineering background really comes into play here because I was able to experience not just biological aspect but working towards the engineering aspect. And the final goal for bioengineering is to apply it to the human condition. So in that sense it was really helpful for me to sort of bridge the gap between, for example, the way — the language a physicist might use compared to the language that a biologist might use, compared to the language that a modeler might use. In that case sometimes people are talking past themselves and they don’t even realize it because they’re not talking in the same language.
Host: Right.
Zarana Patel:So it helps to sort of communicate between these different kinds of mindsets.
Host: Right. You guys are experts in your fields, and so you have kind of your own jargon. Then expert with his own jargon is trying to tell you, that person, you know, his or her perspective and maybe kind of you’re not speaking the same language. That makes a lot of sense.
Zarana Patel:Yeah. And, of course, at NASA we use — on top of that we use acronyms to confuse people additionally. But, you know, I think a great example of just how complex the radiation issue is, is if you think — if you go back in your mind to this very small ion, that’s a physics level here. So you’re involving physicists — both basic and applied physicists. And as it encounters DNA and is doing all this damage, you’re looking at chemistry, radio chemistry. So now you have a radio chemist come into play here. And then you propagate your damage into the cells into multiple tissues, you’re at a biological level here. And then these multiple tissues are interacting in the whole body system. You’re at a clinical level. And you have to take all of these things into consideration when you’re, you know, doing vehicle design, doing mission architecture, doing radiation mitigation and countermeasure planning.
Host: Well, let’s go back to your expertise, which is in bioengineering. That’s something that’s a little bit over my head. What does bioengineering kind of — what’s that field look like?
Zarana Patel:I chose bioengineering because it is — it is this attraction of being able to do whatever it is you want to do. Bioengineering really takes biology and then aspects of any kind of engineering. So if you’re really interested in computers, you could do data informatics. You can weed out data — and data informatics is actually a huge field right now because there’s a lot of data that people are collecting and we don’t know how to weed it out in terms of genomics, proteomics, transcriptomics. And we have to have people who are smart enough to take these datasets and weed out data that is important versus data that is noise and so on. So that’s computer systems engineering. If you want to do something like mechanical engineering — for example, let’s take 3D printing. If you want to 3D print a thumb or a hand for someone, that requires not just mechanical engineering but ideas for — that requires not just mechanical engineering but the concept of biomechanics as well.
How do you fit this mechanical thing you’ve created to the human that you’re going to need to use it for? So that’s mechanical engineering. Electrical engineering is also a huge, huge field with bioengineering. And these memory chips things you can plant in yourself or on yourself, right, to do telemetry, to do telemetry diagnosis for yourself. For example, if I wanted to slap a sticker on myself to measure my sweat — saline concentrations or my sugar levels, they’re developing things to do that as well. Bioengineering has this huge potential that you can target it to whatever it is you want to do.
Host: Yeah.
Zarana Patel:As long as you apply it to the human condition.
Host: Right, yeah. It seems like how does — that’s exactly it — how does technology fit with biology? That’s really — that sounds like kind what it is and meshing those two field.
Zarana Patel:Yeah. And how can you use technology that’s available and modify it to advance the human condition?
Host: So how — how does this help with your understanding of radiation and how that affects the human body?
Zarana Patel:I think it’s just in the sense that I had a perspective of the multidisciplinary nature of things that you can apply to the radiation problem, which does span this huge gap, not this huge spectrum from physics to clinic.
Host: So then — so you’re field in bioengineering really kind of helps you to understand the effects mainly it sounds like the human body. That’s really — that’s really the focus here. Now, I’m sure radiation has impacts on some engineering components, too, and structure and whatever. We’ll focus mainly on the human body. Now, as we’re going to destinations like the moon, like Mars, what is the radiation environment like? Let’s go — let’s skip the moon for now and go to Mars; what is the radiation environment like on Mars?
Zarana Patel:So on the surface of Mars, actually the dose rates are going to be similar to what the crew on ISS will see. The composition will be a little bit different, but the dose rates are very similar. So ISS, you’re getting a lot of shielding from the Earth’s magnetosphere, so you don’t get the lower energy GCR, but you do get a potential for solar flares and you get some higher-energy GCR. If you move outside of ISS orbit to the moon, your dose rates are about one and a half times that of the ISS. Then you go to deep space, that’s where you don’t have any protection from the magnetosphere or a planetary body. You have risk of solar flares and you have GCR, which is always present. So your dose rates can range from two to three times that of the ISS. That is where you’re accumulating a lots of the dose. Once you get to Mars, Mars has an atmosphere that can provide some protection. It can also provide protection just by its planetary body system.
So it can shield some GCR in that sense, which is why the dose rates, again, come down to approximately the same as the ISS.
Host: So it’s mainly — that’s interesting. I always thought that the radiation environment on Mars was much worse. But I guess if you take all of these different things into perspective, one thing that I thought was curious was just being on a planetary body or even the moon — being on the moon gives you a little bit of protection. How’s that working?
Zarana Patel:Exactly. It’s called planetary shielding because you have a sphere and the GCR is just always present. It’s omni present. So it’s surrounding the sphere. But if you’re on the surface of the sphere, wherever the planet is building you from the GCR is where you’re getting protection from it. So the ground itself provides some protection from GCR. And that way you’re only getting GCR from maybe 180 degrees.
Host: So I guess what’s nice about Mars is that it is a planet. So I guess there is that element of being a planet and you don’t have that radiation coming from the other side. Could you maybe burrow underground and use more of the planet to give you more protection? Will that work?
Zarana Patel:Yes, for sure the planet dirt — I think it’s called regolith — you can use that as a shield around yourself. But you also have to account for these things called secondary particles. So any particles that make it through and impact the dirt that your surrounded by will fragment in that volume and create additional secondary particles. So they interact more and more whether it’s shielding or the structure of your house or the dirt that you’re surrounded by. They’re going to generate secondaries that can still impact you biologically speaking.
Host: Regolith, though, is regolith — I thought that was on airless bodies. Is that just the moon or is it — is it — I guess Mars, is that soil?
Zarana Patel:Yeah.
Host: Is that how it works?
Zarana Patel:There’s Martian regolith, there’s lunar regolith.
Host: Regolith. Okay, okay. Yeah, so that — that just gives you just that little bit of protection. So maybe, yeah, would that — if you’re let’s say a mission to Mars, let’s just say around three years in a mission profile. You’re going out, say, nine months transit. You have to stay there for upwards of a year. I guess using the planet around you to reduce that amount of exposure, now that buys you a little bit of time. Because, you know, you said as you’re out in space, the clock is ticking for how much exposure — radiation exposure you’re getting. Maybe that will get you a little bit of extra protection.
Zarana Patel:Yes, for sure. The problem is when you go and come back is where you’re getting the largest dose.
Host: Yeah.
Zarana Patel:And the shielding there is going to be difficult on the vehicle. Because it will require a large mass of shielding and it is not likely to be cost efficient.
Host: Yeah, so okay. So let’s go there. Let’s go to the interplanetary part. This is where the — you’re getting three times the amount, I guess, of — is it three times the amount of Earth or three times the amount of ISS?
Zarana Patel:Three times the amount of ISS.
Host: Of ISS, okay. So three times the amount. So this is where you’re going to have that largest impact. What sort of technology can we look at? Let’s say — let’s take away realistic technologies for a while and just say what is the technology that’s required, that is going to provide you radiation protection?
Zarana Patel:Well, if you can get there faster, that’s probably the biggest thing.
Host: Sure.
Zarana Patel:Because that minimizes the time you have to spend in space.
Host: Propulsion.
Zarana Patel:Propulsion is going to be the big one. There’s also been talk of magnetic shielding. Maybe I didn’t mention, but GCR is not on the electromagnetic spectrum. So on the electromagnetic spectrum you have wavelengths that — on one end you have very large, long wavelengths with low frequencies, things like radio waves and microwaves that you mentioned. And then you progress to higher and higher energies and higher and higher frequencies. So the light that we see is on the visible length spectrum — visible light spectrum. And then you have UV spectrum. And within this UV spectrum you have delineation between non-ionizing and ionizing radiation. So basically, ionizing radiation just means that the radiation has capability to excite an electron and to knock it out of its — out of the orbit of the whole nucleus. And non-ionizing radiation doesn’t have that capability. So within the UV spectrum, UVA and lower-energy UVB wavelengths are considered non-ionizing.
And then the higher-energy UVB and all of UVC is considered ionizing. And then after — after beyond the UV spectrum you have X-rays and gamma rays, which are the highest energy, highest frequency wavelengths. And those are definitely ionizing. But GCR, galactic cosmic rays, aren’t even on electromagnetic spectrum. They are technically not even rays. As I mentioned, they’re heavy ions.
Host: Right, right
Zarana Patel:Electromagnetic wavelengths carry their energy in these little packets. They carry their energy in these little packets called photons. And photons can act as both light and wave particles. But GCR is a ion, it’s a particle. And it has a mass, it has an electric charge, and it can be affected by magnetic fields. So it is definitely ionizing, but it is not an electromagnetic wavelength. So if you consider shielding, if you — if you want to have some kind of magnetic shield, it could potentially disrupt the GCR field around the vehicle and in a way that sun does or our Earth magnetosphere does to protect us.
Host: Ah, okay. So generating sort of like a small, I guess, magnetic field.
Zarana Patel:I’m not sure that there — I’m not really sure about the details of it.
Host: Oh, okay.
Zarana Patel:But when you — when you project a magnetic field around a vehicle, that in turn will disrupt the GCR flux that comes in. So I don’t think it’s — the interaction is generating the field. I think you have to generate the field and then that protects you.
Host: Okay. I heard that water was a really good one, too.
Zarana Patel:Yes. So things like water or polyethylene are really good shielding. And the good news is you’re already going to have water on the vehicle. You’re going to have to carry your water. So there are — there are schematics where, for example, for a solar particle event you would go into one — one area and surround or repack the water bladders around your habitat so that you could provide temporary shielding that way.
Host: Ah, okay. So a solar flare has happened. We can detect it a little bit early. We got a little bit of time before we know it’s going to hit the spacecraft. Then they get word, “Hey, shelter.” So they go and surround themselves with water.
Zarana Patel:Exactly.
Host: Okay.
Zarana Patel:The problem is that it’s probably — the water shielding is not sufficient to protect from GCR. So you would need a lot of — a lot of depth of water or polyethylene, which just isn’t going to be realistic.
Host: Right, yeah. You’re not going to be a bring a pool with you to Mars.
Zarana Patel:No [Laughs].
Host: Okay. So — so let’s go back. We kind of mentioned I think briefly some of the effects that we know that are the cause of radiation or at least have some sort of impact. Going down the list, one of them was the cardiovascular system. What’s happening there?
Zarana Patel:So that — that is a great question. What we think is happening is that radiation in general, whether it’s gamma rays or GCR, is causing endothelial dysfunction. So your vessels have different layers within them, and one layer is called the endothelial cells. And this is the layer that interact with the blood. And when you have dysfunction of this layer, you can start creating barrier dysfunctions within it. You can also start creating adhesions of macrophages and immune cells, and that’s the first step in atherosclerosis. Basically, you’re laying down plaque into your arteries. And when you have the endothelial barrier disrupted, you start this process. So this is what we think is happening with low levels of space radiation, but the research program we have in place is doing a lot more work to characterize if that’s exactly what’s happening.
Host: Now what about — you said there was some effects on the brain, too? You mentioned Alzheimer’s. But one thing I was thinking of is, I guess, more of a real-time effect, I guess, if you’re getting blasted these particles. Could it potentially affect your mood and your emotions or the way that you interpret information? Anything like that happening in the brain?
Zarana Patel:Yeah, there is a risk for in-flight CNS decrements to happen. And so the research to date that we’ve had in animals suggests that, you know, at low doses similar to what you might see in the Mars missions, you can potentially generate these kinds of decrements that can then go on and translate to mission-affecting behaviors. Whether or not that’s actually going to happen is something that the research still has to play out. And I think that Dr. [inaudible] can talk more about that.
Host: Okay, okay. Yeah, he’ll be next in our series, so that will be great. Thinking about some of the — we were talking a little bit about the ways that we can protect from radiation. But like you said, this is a phenomenon that’s all around us. It’s, you said, omnipresent. Is there a way that knowing that radiation might have — it’s going to have an effect. You know, if we send astronauts below low-earth orbit, it’s going to have an effect. Is there something we can do to maybe reverse the effects or anything to sort of help reverse the effects of radiation?
Zarana Patel:Yeah. So within our research, we’ve noticed that the commonality among these risks is — there is one commonality, and the commonality is chronic inflammation. So something that targets inflammatory pathways would be a good first step to identifying countermeasure. Right now we’re looking at things like aspirin and antioxidants. Those are the first tier. These are — these are categories of drugs that have already been clinical proven on the ground for safety and efficacy and in clinical trials. So there are FDA-approved drugs that you can use in case of these large accidental exposures for acute radiation syndrome. And that’s a tier two drug that we can also consider. The third type of drug is drugs that are being investigated to mitigate radio toxicities after cancer therapy. So in the clinic when people are getting radio therapy, they are going to experience heart disease later on in their life. They’re going to get secondary cancers from that radiation. And there’s a huge field NIH is currently funding to develop mitigators for those radio therapy-induced toxicities.
And the fourth is very specific to space radiation: Are there drugs that we can use to target mechanisms or pathways that are space radiation-specific versus gamma or X-ray radiation-specific?
Host: These heavy ion ones?
Zarana Patel:Mm-hmm.
Host: Yeah. Yeah, yeah. Now, one thing was talking about — we’ve talked a little bit about the effects, you know, cardiovascular things that are happening to the human body, and these interdisciplinary efforts. You know, looking at not just radiation. One of them you mentioned was cataracts and eye damage. I know just from talking with a lot of other experts that there is a — there is a challenge with vision problems in astronauts just from being exposed to, I guess, the microgravity environment. There’s this fluid shift that happens, and there’s a lot of other factors that may contribute to this. Now, radiation sounds like it’s kind of an effect of its own. What are we learning there of how these disciplines are crossing and affecting the eyes?
Zarana Patel:The thing about cataracts and astronauts is that it’s been long established as an effect of space radiation. And it’s actually the one biological effect we know and we can see and identify and point to as a space radiation effect in this small astronaut cohort. They get it, we know it’s from space radiation, and we know that we can mitigate it very easily. It’s a simple — relatively simple surgery.
Host: Surgery.
Zarana Patel:So it is a known space radiation effect, but NASA quantifies it as a acceptable risk because the surgery for cataracts is fairly simple. It also manifests later on in life. And so it’s not an in-mission risk. So the thing with the SPANS risk, which stands for space flight-associated neuroocular syndrome, is that it’s been only identified recently. Now, there’s still a lot of data to be collected from that. They’re not sure if it’s caused by microgravity, if it’s caused by fluid shifts, if it’s caused by something else — elevated intercranial pressure. So the — there may or may not be some kind of interacting with radiation as well. We just don’t know yet.
Host: Yeah. Now, one thing about being a scientist and, you know, you’re working in the NASA Space Radiation Laboratory, trying to get data points to understand what is happening, we’re looking forward to going beyond low-earth orbit new. You know, we’re talking about missions on the moon, missions to Mars. Let’s go to the moon for a second and let’s assume we’re in the middle of a long-duration stay on the moon; what scientifically from a radiation perspective and a biological perspective are you looking forward to?
Zarana Patel:So a lot of the samples, the data we get from astronauts and crew involves blood samples. And what we can gather from those samples is are there any chromosome aberrations within those samples? What kind of DNA damage is happening? So I think that is a, one, very useful tool. We call it biodosimetry. So it’s a biological measure of the dissymmetry, the radiation dose that you’re going to get. I think the biodosimetry from a long-duration mission — long-duration mission on the moon would be really useful. We don’t have that data yet. Other things that would be interesting to look at are same thing in the blood samples, looking at biomarkers that are of interest for all four of our risks. So cancer, CNS, and cardiovascular disease. Other things that we could look at would be the cardiovascular morphology, doing an echocardiogram on the heart. Or doing an MRI on the brain or even on the heart itself to look and see if there are early markers — subclinical but early markers that we can use to identify potential downstream effects and mitigate them earlier.
Host: Yeah, so a lot of data that we can get, really, and to help us understand the environment. So can you tell us about some of the more recent studies that you’ve been doing for in terms of radiation, maybe in the NASA Space Radiation Laboratory?
Zarana Patel:Yes. We are planning — so NSRL actually has three runs a year, spring, summer, and fall. And this fall, 18C we’re planning to do the first test of our GCR simulator. So we’re going to irradiate animals and test out this scheme that we have to simulate the space radiation GCR field. We’re going to irradiate them with — six days a week we’re going to irradiate them with this schema, these five ion beams because hydrogen and proton, and we’re going to see what happens to these animals over varying lengths of time. And in that way we hope to simulate a three-year Mars mission and the endpoints that we might see in the human cohort.
Host: Hmm. Okay. So yeah it’s coming up this fall. Where — where is it again? Is it on — here at NASA?
Zarana Patel:Yeah, the Space Radiation Laboratory is housed at Brookhaven National Laboratory. It’s on Long Island.
Host: Long Island? Okay. So you’re going out to [inaudible].
Zarana Patel:Yes [Laughs]. Yeah, they have a — so Brookhaven National Labs has a very large linear accelerator. And what they do is they pull off a little bit of the large beam and route it down to NASA Space Radiation Laboratory. And that’s a very simplified way of what’s happening with all the aspects of it [Laughs]. But in that way that we can then sort of piggyback off the large lunar accelerator.
Host: Yeah, it’s not — you know, when you say, “Oh yeah, we have to simulate this galactic cosmic ray, this galactic cosmic background radiation” that’s not an easy thing, it doesn’t sound like.
Zarana Patel:No, it’s not easy at all. And as I said, this is probably the only facility in the worlds that is capable of doing it to date.
Host: Wow. Yeah, we were talking — we were talking [Laughs] a little bit about everyone always asks us, you know, “Where is your zero-G room?”
Zarana Patel:Yeah [Laughs].
Host: [Laughs] Like we have a room where you can just sort of flip a switch and oh yeah, we’re in microgravity. It’s so much more complicated than that when you get into it.
Zarana Patel:Yeah, you have to take every ground analog with a grain of salt obviously. But you also have to use what you can with the limitations of only being able to send a limited number of people for a limited number of times into space with a limited budget.
Host: Yeah. Now, I know there’s a lot of ground analogs here. There’s — you know, some are sort of simulating a Mars habitat. You know, you’re living in space, I guess, simulated for X number of days, whether it’s, you know, HERA does 45-day missions now, there’s the Mars 500, you got Antarctica.
Zarana Patel:Yeah, things like HERA where they take a crew of three or four people and they isolate them in a similar vehicle type format for varying numbers of days, you know? I think they started at, like, something like five days and now they’re up to 45 days. You can really get a feel for how does — how do some of these other hazards like isolation and confinement affect the human? And not just the human but their interactions with other humans.
Host: Oh. Is that [Laughs] — this kind of goes back to that what’s happening with the radiation and how it affects our mood; can you imagine if you’re in this closed box with, you know, five other people on a journey to Mars and all of a sudden this radiation is making you [Laughs] antsy or anything like that? That would be — that would be unfortunate.
Zarana Patel:Yeah, so the risk of radiation versus the risk of behavioral health and performance, it’s going to be a really difficult issue.
[ Multiple Speakers ]
Zarana Patel:For me, I got sucked into NASA very early on because I love to read. And my brother sort of introduced me to sci-fi. And in that moment I was hooked. So I read all the sci-fi greats. I read Asimov, Bradbury. And for me it is really this long-term goal of manned space flight and exploration to the cosmos.
[ Multiple Speakers ] That is worth the risk.
Host: Yeah, there’s still a lot to explore. I mean, just recently, Scott Kelly spent a year in space more than any other NASA astronaut before him. And that — he gave us a good perspective of the [inaudible] missions and the time that we’re I guess allowed or supposed to spend in space [inaudible]. Is there anything you know based on that study [inaudible] longer period of time in space will do from a radiation perspective?
Zarana Patel:Yeah, there was a lot of discussion about how Scott, when he came back, the whole event changed his genes. And I think it’s important to note that his genes weren’t actually changed. Him and Mark are actually still twins [Laughs]. But what did change was the gene expression. So what happens when you live for a year anywhere is that you have the environment that you’re surrounded by change you and then sort of the nurture part of nature versus nurture. So nature is genes [inaudible] change. The nurture part is the environment [inaudible]. It did affect him. So even if you spent a year of your life and you went on a diet or you had sleeping habits change, you had a baby or you changed jobs, you would experience epidemiologic change in that year of life. So when he came back, actually, the level of change that we saw was fairly similar to something like a human might experience in a stressful environment, like if you went scuba diving or if you were climbing Mount Everest.
So nurture is the environment, and within the space radiation environment you’ve talked about these five hazards. There’s isolation, confinement, distance from Earth, radiation. And the whole body outcome is that you’re exposed to all five of these simultaneously. And it’s really difficult to say that one is responsible for these genetic expression changes in Scott. You’re not going to be able to tease that out based on one person. He had a whole body response and it’s similar to someone spending a year of their life in a stressful situation away from family. But with the levels of — actual levels of changes he saw within six months of returning to Earth, most of them went back to pre-flight levels but only 7% persisted to date. So that means that 7% of the gene — the ways that his genes are expressed is changed. And that’s considered fairly minimal. Now, that’s only a year on the ISS, which is a fairly low-dose radiation environment.
You know he’s close to Earth. There are return options. With the three-year Mars missions, there’s going to be increased risk. But I think — I think the risk for — obviously the risk for these crew is worth it. They are willing to go and do these things. And it is hard, but I think we should enable them in every way we can. I think that is the whole point of our Human Research Program.
Host: Yeah. A lot of the guests I talk to is there’s so much that we don’t — that’s, like, a big theme, is there’s so much that we don’t know. So you got to have the bold astronauts that are willing to be, like — you know, raise their hand and be like, “I’ll do it. I’ll be the person where you can study me and figure out what happens to me. And that way we can understand what happens and more people can go.” Because I feel like a lot of people do want to go. There’s a lot of people already signing up. They’re like, “Yeah, I’ll go to Mars.” [Laughs]
Zarana Patel:Yes, for sure. Because the risk is worth it. And if they’re willing to take that risk, then we need to do our best to mitigate the risk for them.
Host: And I’m glad that you’re on the front lines, helping out from the radiation perspective. Zarana, thank you so much for coming on and sharing this perspective of what happens to the human body in the radiation environment. Thank you.
Zarana Patel:You’re welcome. Thank you guys for this opportunity.
Host: Of course.
[ Music ]
Host: Hey, thanks for sticking around. So today we talked with Dr. Zarana Patel about that first hazard, radiation. So we have four more to go. Do you want to see the overview again? Again, the last episode that we did was with Dr. Mike Barratt. And he went over all five hazards. Otherwise you can go to NASA.gov/hrp. We’re working with the Human Research Program here at NASA to put these five episodes together for you. And while we are releasing these episodes, you can go to that website and check out some of the products that they have that are associated with some of these topics. So you can go there right now and check out some of the stuff they have on radiation. Otherwise you can see what we’re doing at the International Space Station realtime research going on at NASA.gov/iss. And then, of course, the social media accounts on the NASA Johnson Space Center and the International Space Station. Go to any one of those accounts. Use the hashtag #AskNASA, mention Houston we have a platform and ask a question [Laughs].
Houston we have a platform — Houston, We Have a Podcast on your favorite platform. There it is. And then [Laughs] ask a question and we’ll put it on the podcast. We’ve done it a bunch of times before and even made whole episodes out of it. So this episode was recorded on June 29th, 2018. Thanks to Alex Perryman, Pat Ryan, Bill Stafford, Bill Polaski, Judy Hayes, Isidro Reyna, Mel Whiting, and Natalie Gogins. And thanks again to the radiation expert, Zarana Patel, for coming on the show. We’ll be back next week with part two of the five hazards of human space flight, discussing isolation and confinement. See you then.